Surgeons acknowledged that nitrous oxide-oxygen anesthesia gave less satisfactory muscular relaxation than either ether or chloroform, required expensive and cumbersome apparatus for its transportation and administration, cost more than other anesthetics, was technically the most difficult to administer of all the anesthetics then available, and was dangerous in inexperienced hands. However, Crile thought these disadvantages to be outweighed by its advantages. Nitrous oxide proved quick in action and pleasant to take; recovery occurred immediately, without nausea; food could be taken soon after recovery; patients could be transported soon after recovery; less nursing care was required; such complications as bronchitis, pneumonia, and nephritis did not follow it. In his shock research, Crile experimented with nitrous oxide and concluded that the addition of oxygen would give better protection to the central nervous system against the shock of surgery than ether or chloroform.
Crile enlisted Agatha Hodgins to administer nitrous oxide anesthesia during the Lakeside Unit’s three month term. “One morning in 1908 while making rounds, I drew Miss Hodgins aside and presented to her what amounted to an annunciation. She had received no warning about the plan to make her my special anesthetist but she told me promptly that she would undertake it if I would remember always that she was giving her best… and I never had any occasion to be disappointed in her work.” Hodgins perfected the administration of nitrous oxide-oxygen.
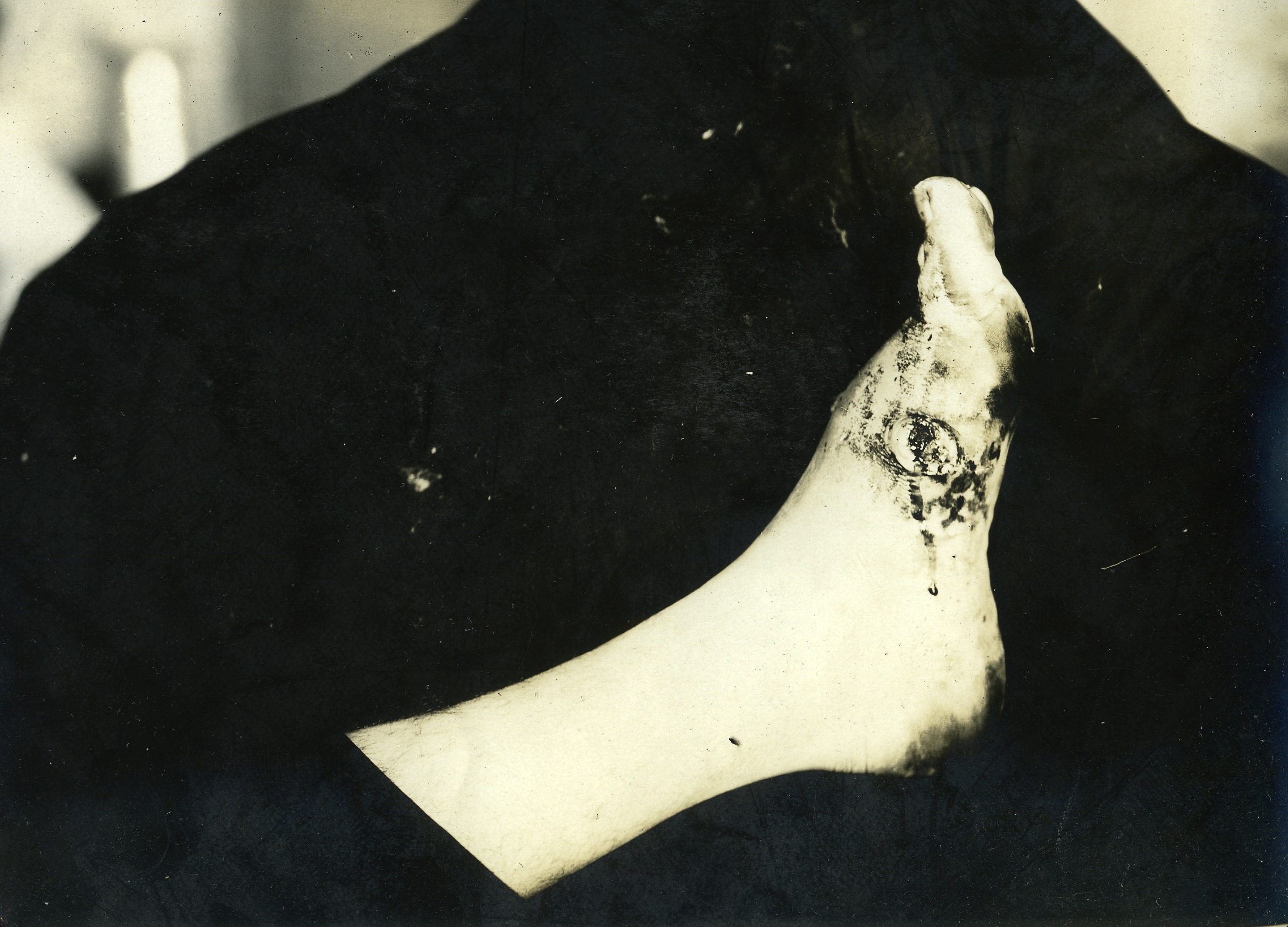
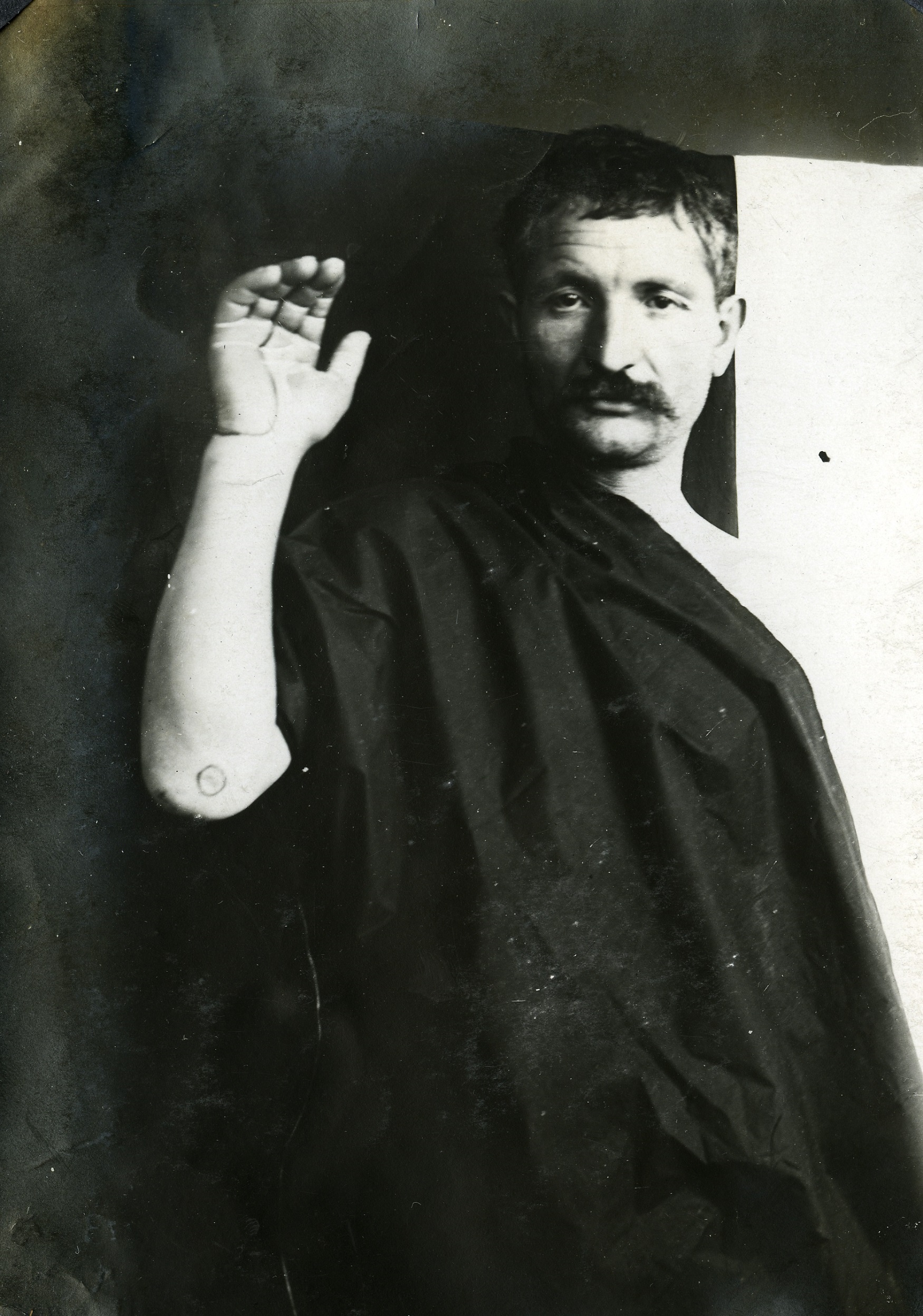
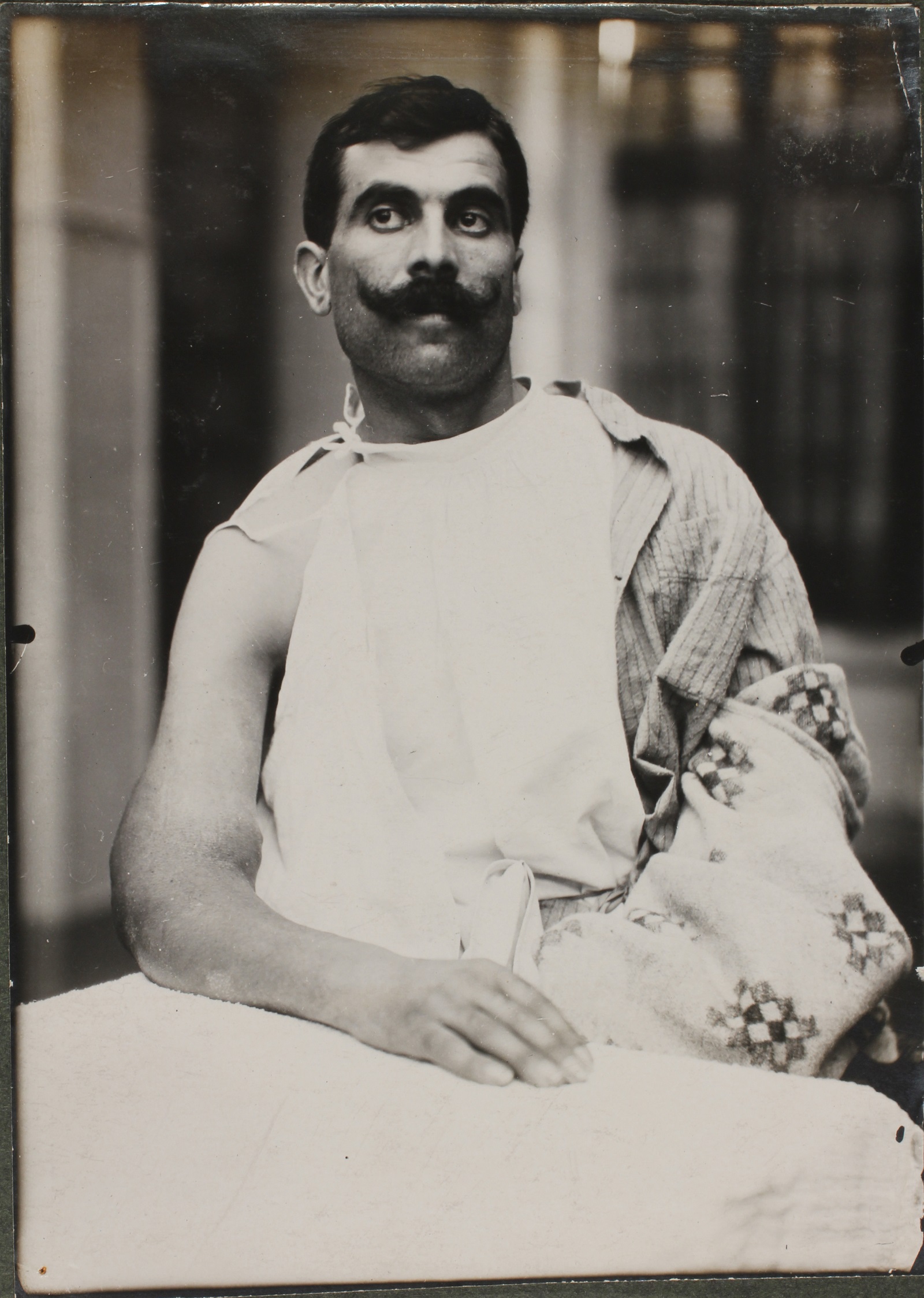
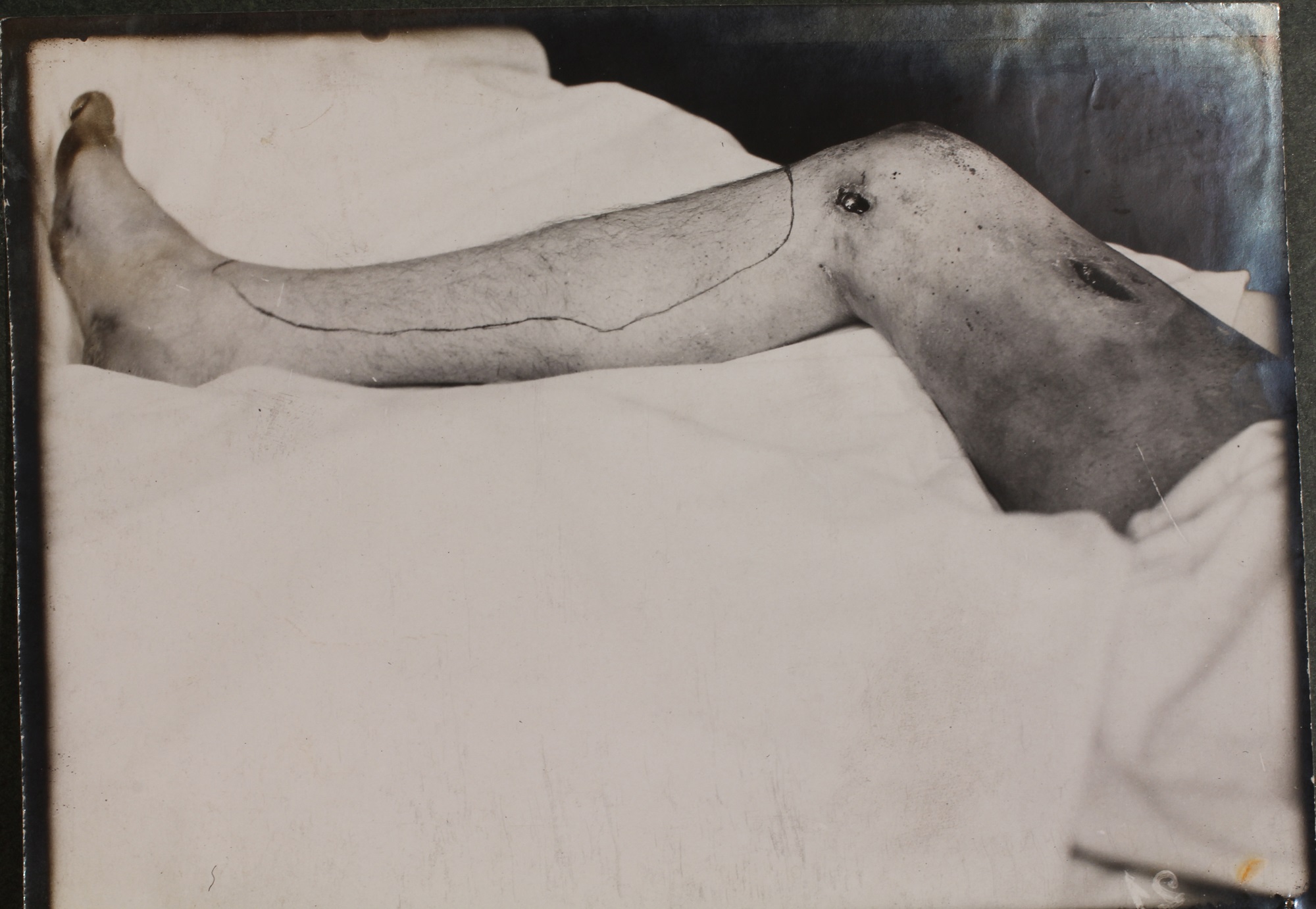
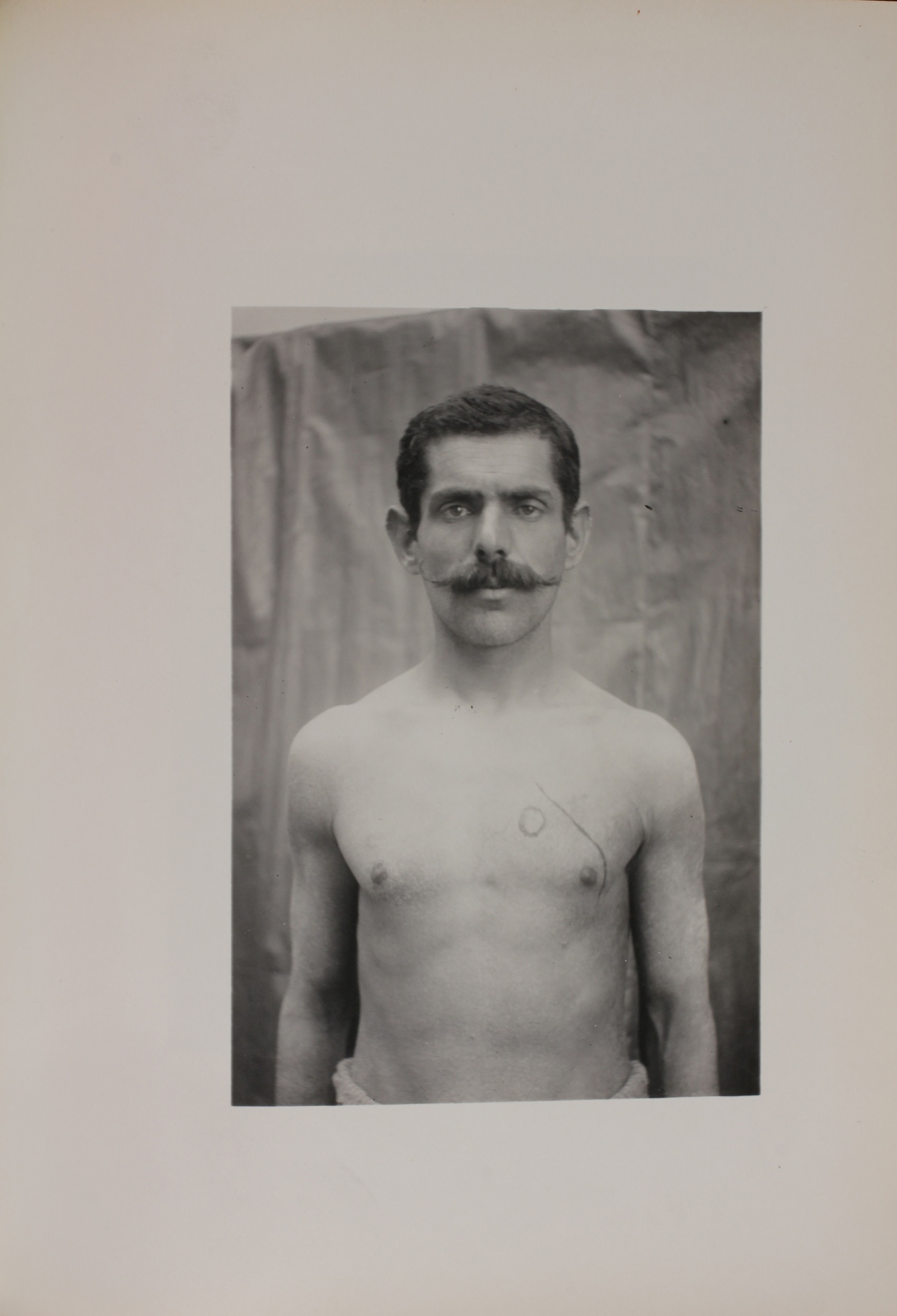
The cases seen by the Unit fell within several broad categories: gunshot wounds, shrapnel and shell wounds, fractures, frostbite and trench foot. At a distance from the front, the American Ambulance received severely wounded soldiers requiring long convalescence. Injured soldiers who reached the hospital had an excellent chance of recovery. The exceptions were patients with abdominal wounds, most of whom died. Tetanus and gas gangrene were relatively rare occurrences. Of the 1200 cases admitted up to March 1, 1915, there were only four cases of tetanus and severe gas gangrene. Chest wounds usually did very well. Although the overall mortality rate was high, those who survived recovered well.
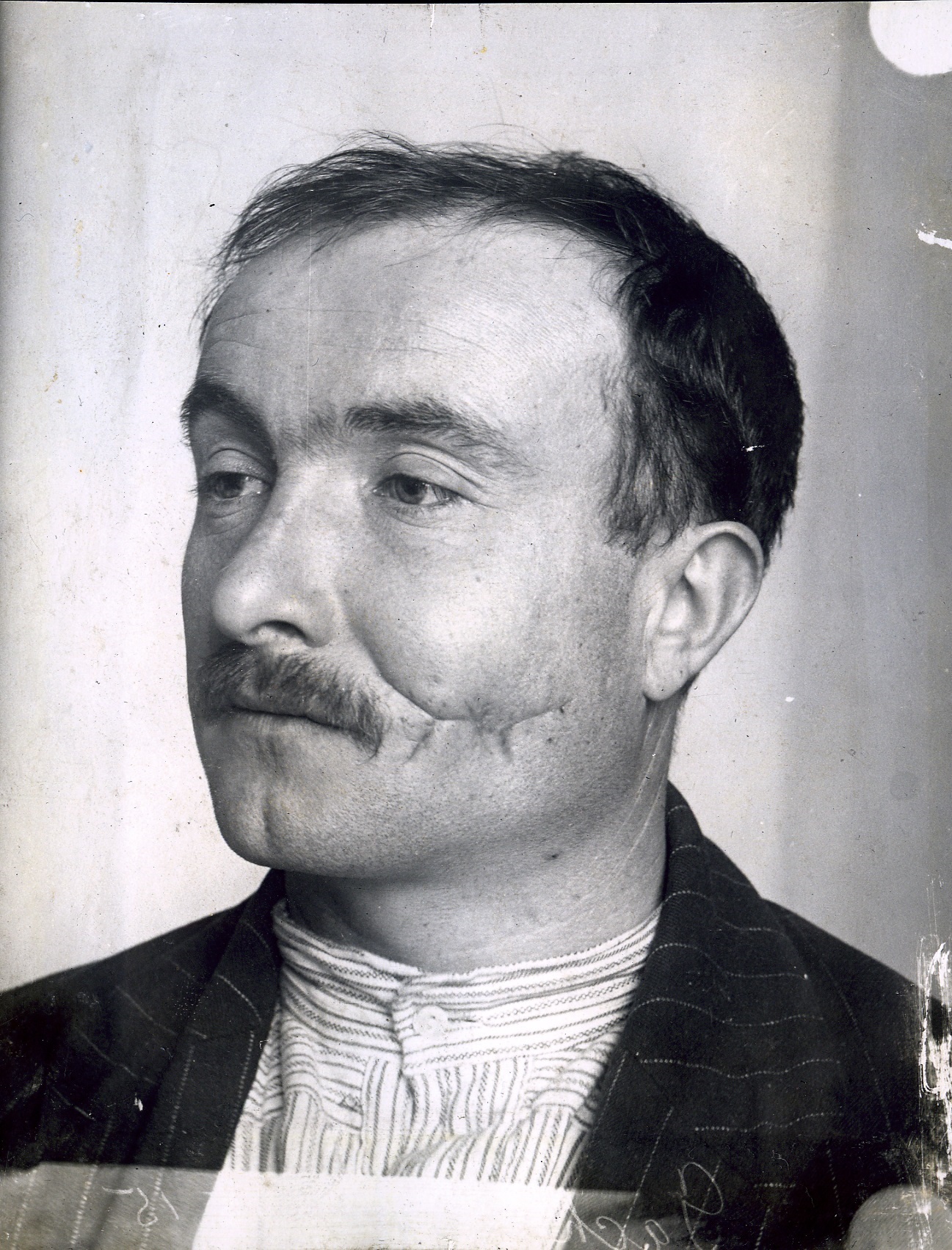
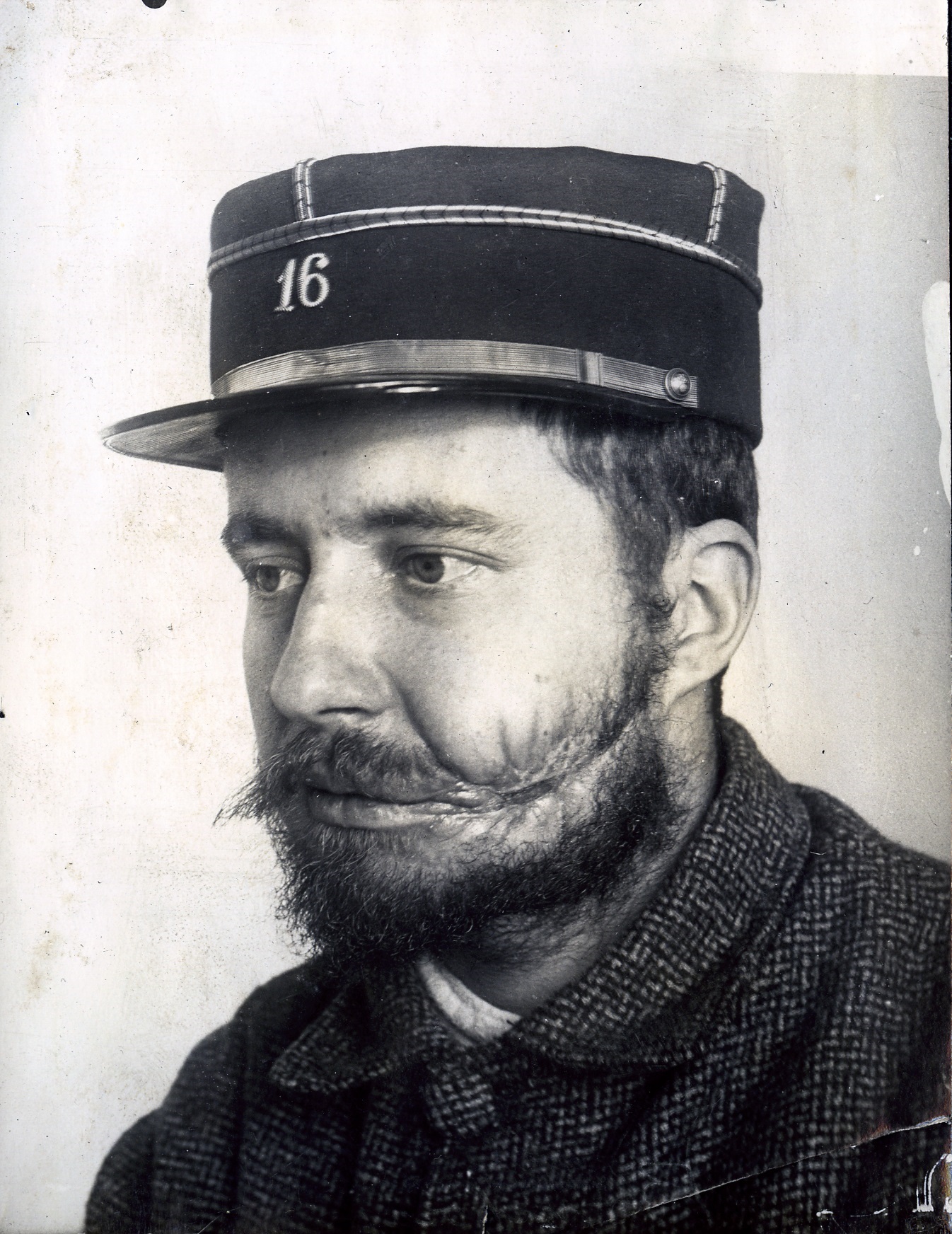
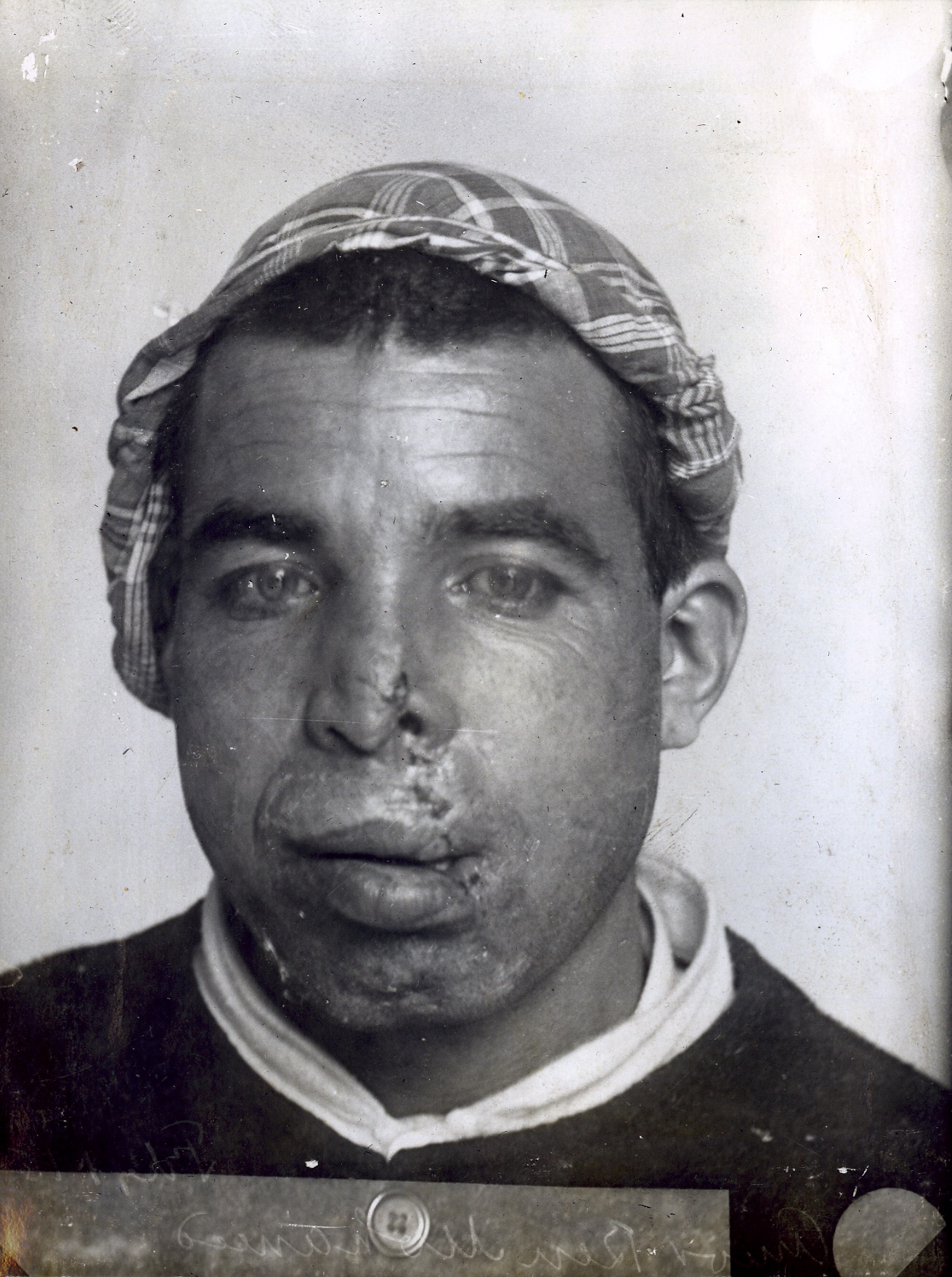
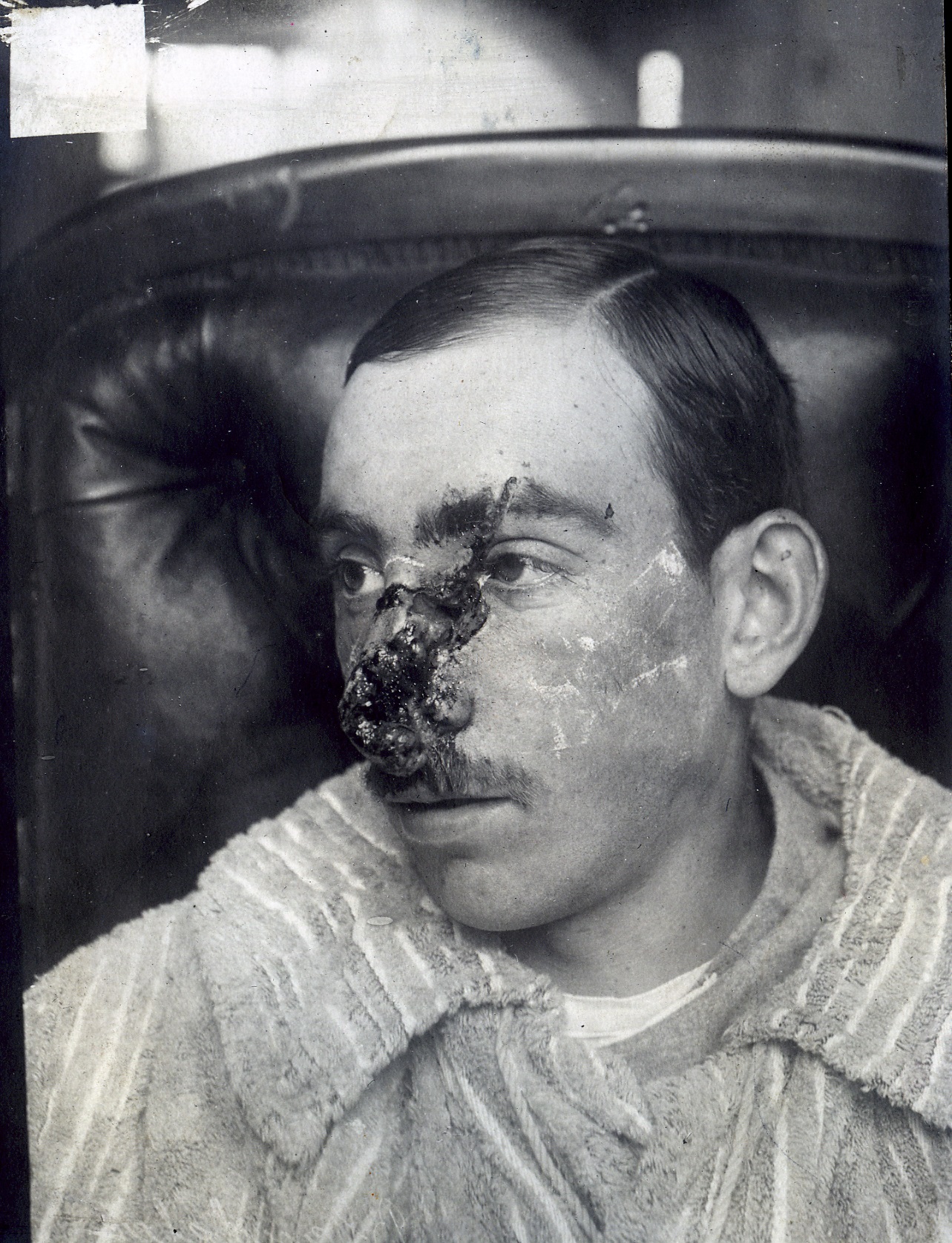
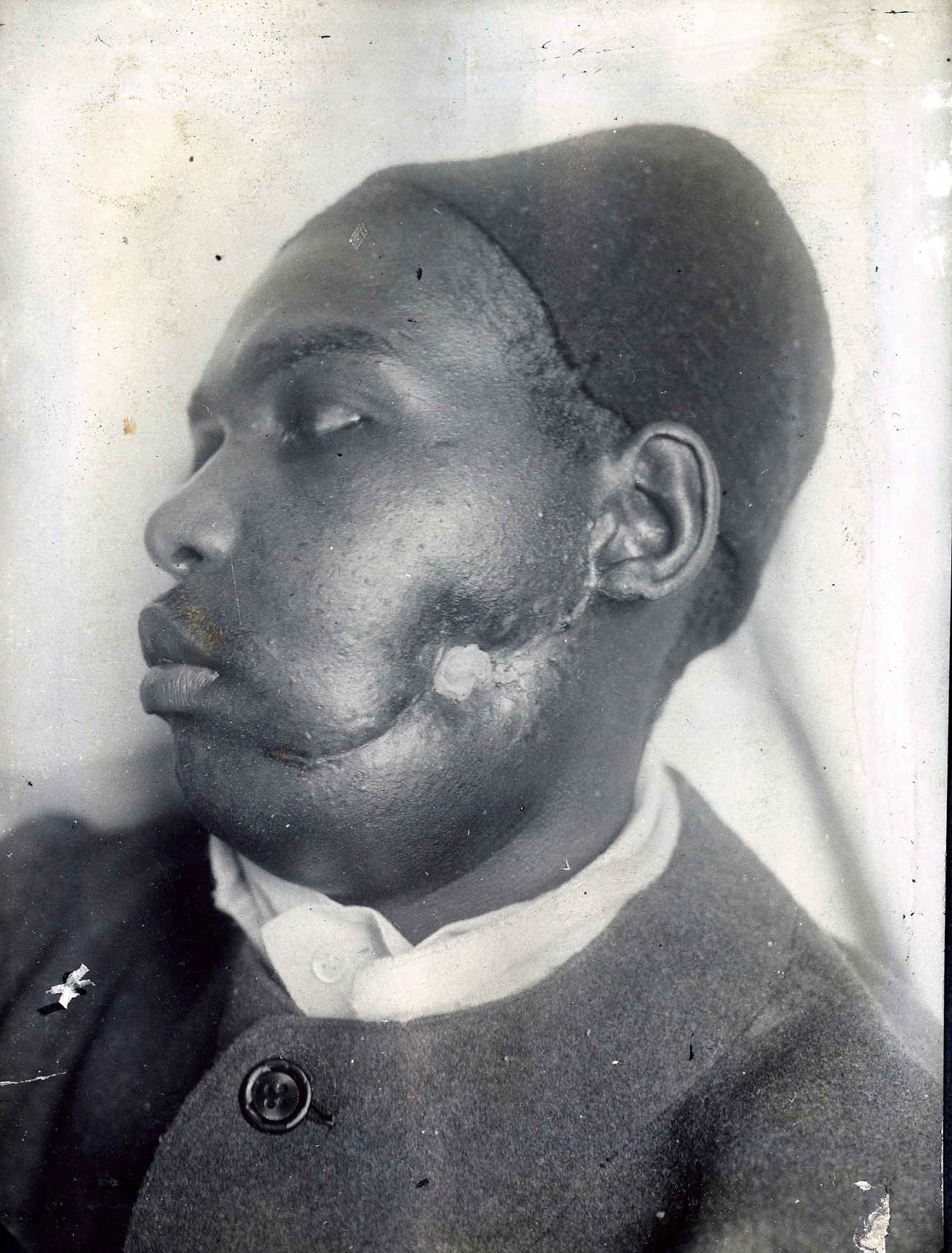
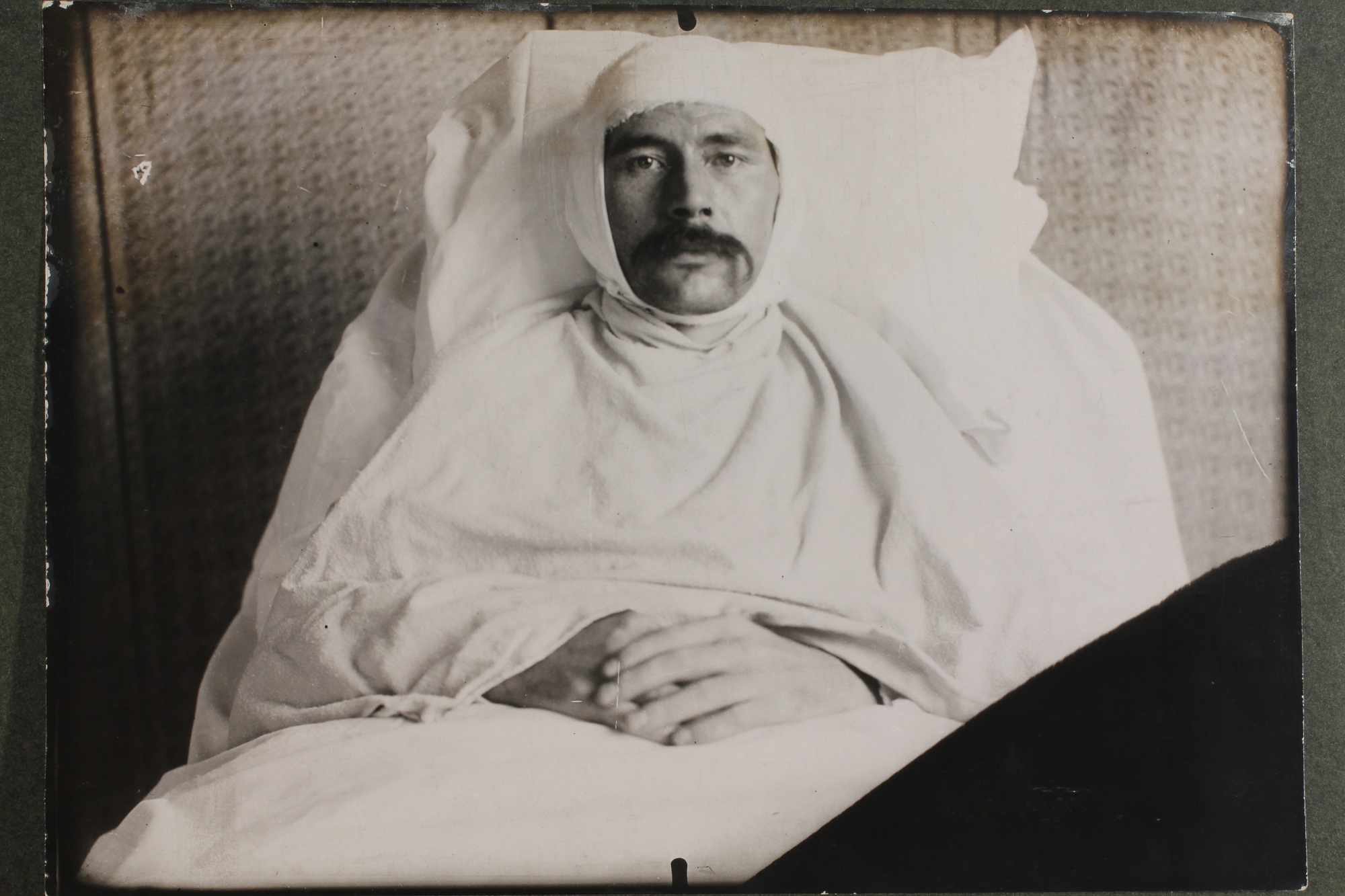
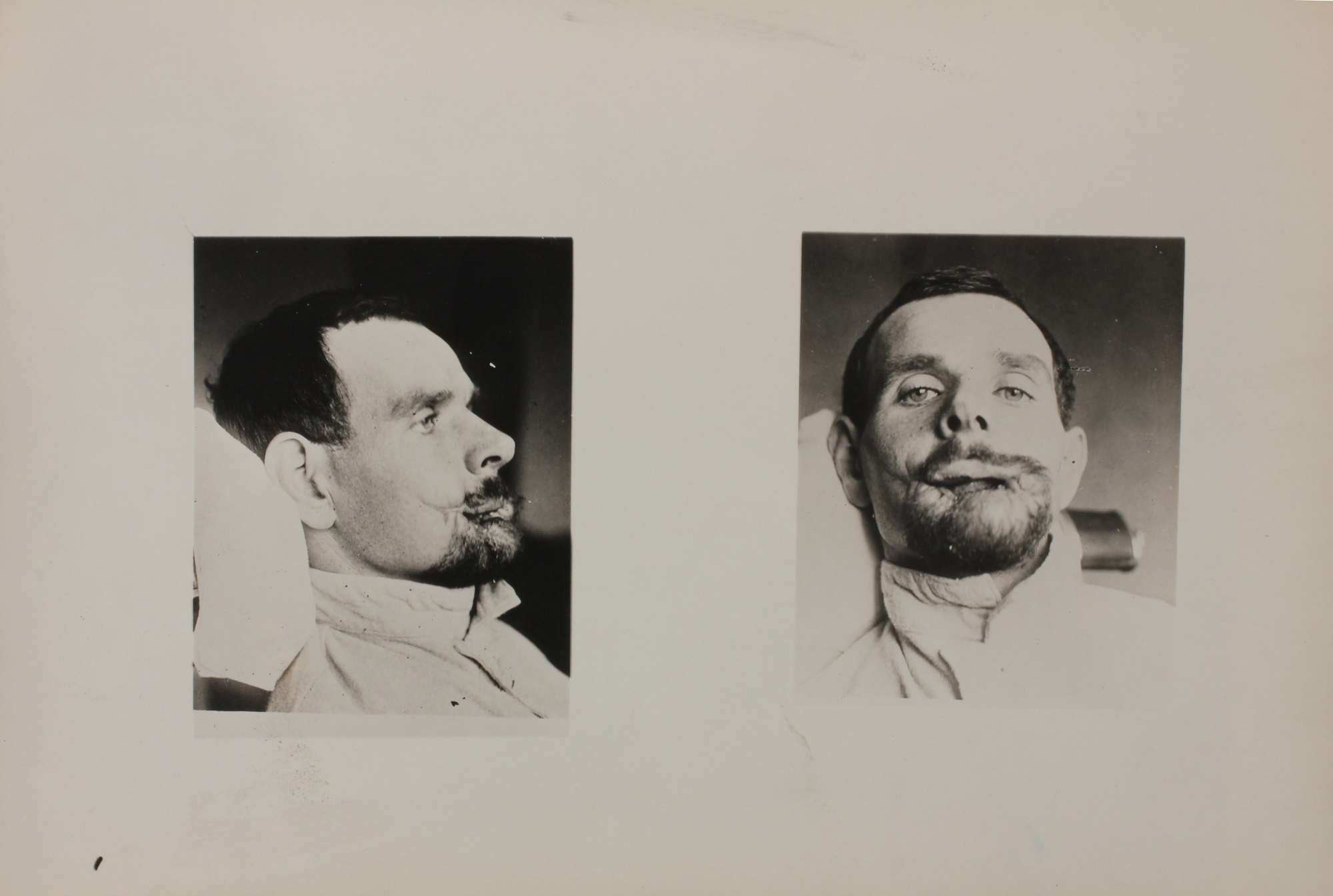
It was noted in reports submitted by American Ambulance personnel that trench warfare was generating an increase in the number of facial and head wounds. Dr. Hayes, Chief Dental Surgeon at the American Ambulance, worked closely with the Lakeside Unit. In his 1915 annual report, Dr. Hayes distinguishes the American Ambulance as being the first military hospital to have a dental surgeon on its medical board. Initially, the dental department spent most of its time examining the teeth of patients to provide general dental hygiene. As these cases of “fractured jaw” were brought in, a new branch of dental surgery and dental orthopedics came into existence.